

Skeletal Fluorosis
The Hidden Burden of Fluoride in Our Bones

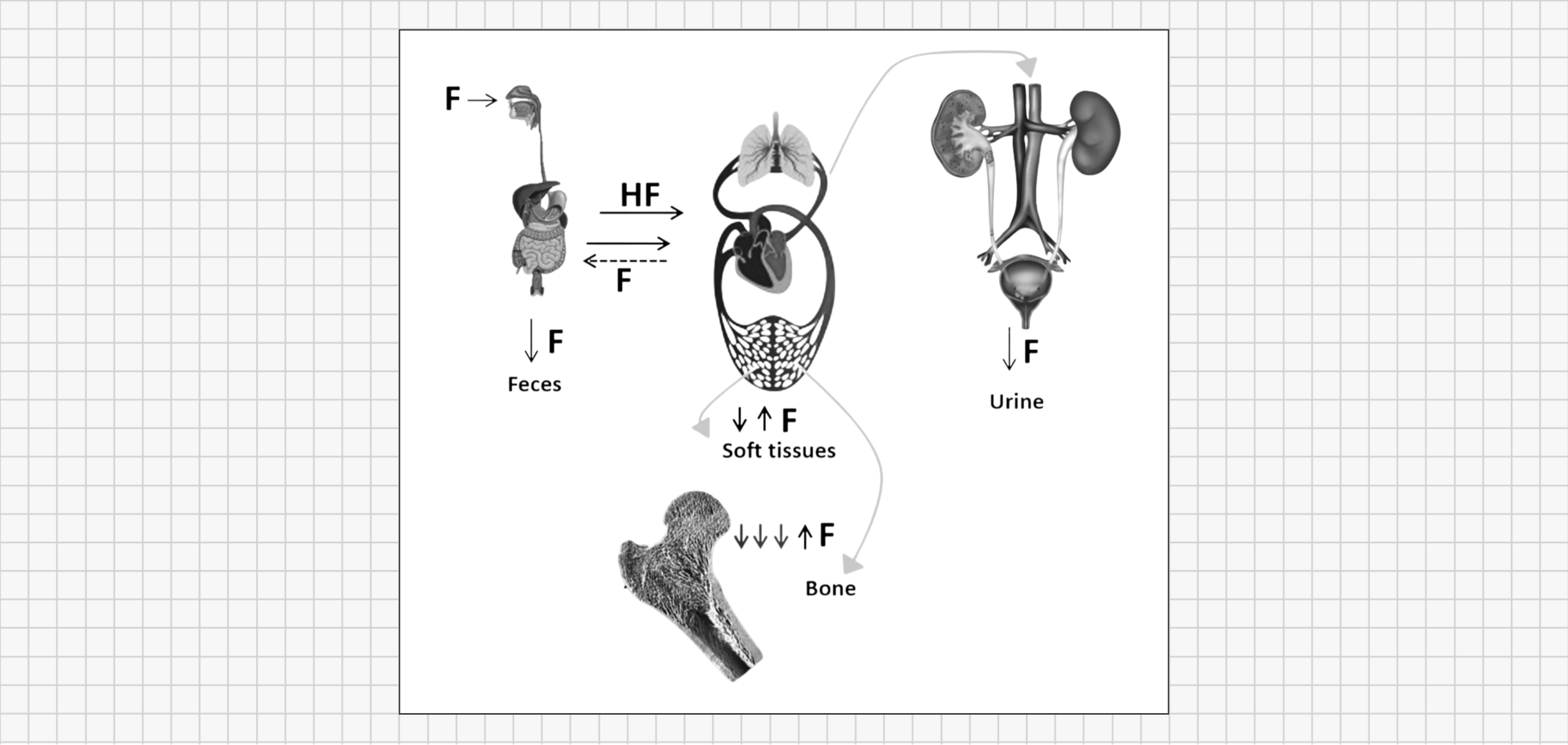
In last week’s issue on Dental Fluorosis, I explained that fluoride doesn’t simply pass through our bodies - it builds up and lingers. Roughly 90% of the fluoride we ingest is absorbed into the bloodstream, and our kidneys only filter out about half of it. The rest recirculates and eventually settles into our tissues, especially our bones and teeth. Over a lifetime, different age groups retain fluoride at different rates:
Infants/children: up to 80–90% (their growing bones eagerly absorb minerals)
Adults: ~50%
Older adults: ~40% (aging bones absorb slightly less)
Because the body has no quick, natural way to eliminate stored fluoride, each exposure leaves a lasting mark. In teeth, that mark is visible as dental fluorosis (mottling or streaking of enamel). In bones, however, fluoride’s effects remain hidden until they manifest years later as pain, stiffness, or fractures.
In this issue, we focus on that deeper hidden burden: skeletal fluorosis, the condition resulting from fluoride’s gradual accumulation in bones.

Contents
Skeletal Fluorosis Explained
How Healthy Bones Are Built
How Fluoride Changes Bone
The Stages of Skeletal Fluorosis
Why the Damage Lasts a Lifetime
The Silent Burden and Misconceptions
How To Reduce Your Risk

Skeletal fluorosis is a chronic bone and joint disorder caused by the gradual buildup of fluoride in the skeleton. Over years of continuous exposure, fluoride accumulates in bone tissue and disrupts the normal cycle of bone renewal (remodeling). Early on, these changes are microscopic and cause no obvious symptoms. But over time, subtle damage accumulates into serious structural problems: bones slowly lose their natural resilience, becoming harder but more brittle, and joints gradually lose flexibility as ligaments and joint tissues calcify.

To understand how fluoride affects bones, it helps to understand how healthy bones function. Bone may seem rock-solid and unchanging, but it’s actually living, dynamic tissue. A healthy bone has two main components working together to give it both flexibility and strength:
A flexible framework: Roughly half of a bone’s volume is a matrix of tough collagen protein fibers. This collagen network provides a bit of bend and stretch, so the bone isn’t too brittle.
Hard mineral crystals: The other half of bone is made of tiny calcium phosphate crystals (hydroxyapatite) that deposit around the collagen fibers. These mineral crystals harden the structure, giving bone its rigidity and load-bearing strength.
Throughout our lives, bones constantly renew and repair themselves through a process called bone remodeling. In this process, specialized cells work in balance: osteoclast cells break down and remove old or weakened bone (resorption), and osteoblast cells build new bone to replace it.
Under normal conditions, this removal-and-replacement cycle stays in equilibrium – the amount of bone removed is about equal to the amount rebuilt. This continuous remodeling repairs minor damage (like tiny stress cracks), adapts bone density to our activity level, and maintains proper bone structure.
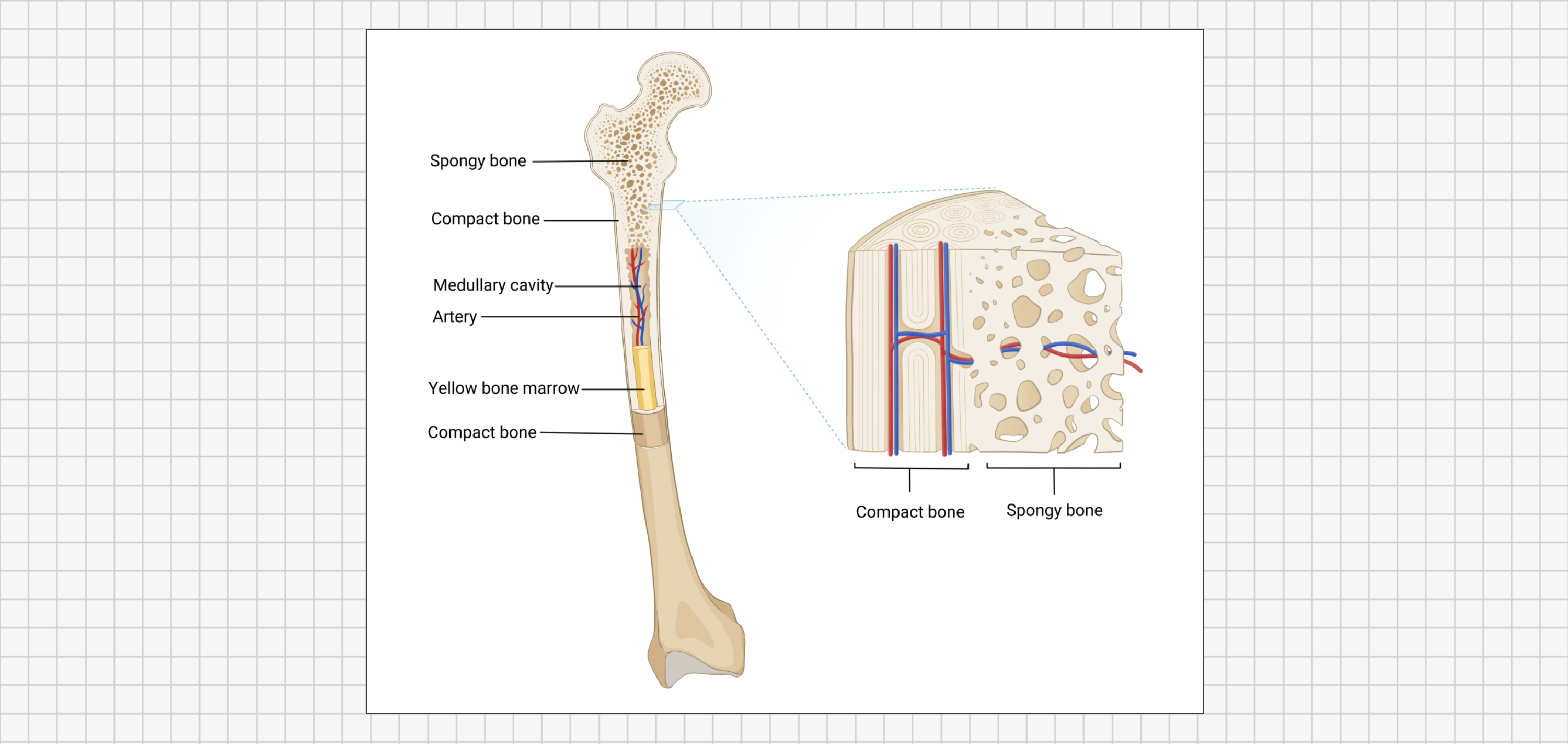
For example, consider a weight-bearing leg bone. It has a dense outer layer of compact bone for sturdy support, and a spongy inner layer of trabecular bone near the joints to help absorb impacts. Both types rely on proper mineralization (the right deposition of calcium and phosphate) alongside the collagen matrix to stay strong yet slightly flexible.
In essence, healthy bone strikes a delicate balance: it is rigid enough to support us, but flexible enough to bend slightly under stress without breaking. If the remodeling process is disrupted, or if something alters the composition of the bone’s mineral crystals, the bone can become either too fragile or too inflexible (rigid).

When fluoride enters the body, it doesn’t just float around harmlessly - it has a strong affinity for calcium-rich areas, and our bones are the largest calcium reservoirs we have. Fluoride ions readily bind with the calcium in bone. In doing so, fluoride actually becomes part of the bone’s mineral content, forming a compound called fluorapatite - essentially a fluoride-enriched version of the normal bone mineral (hydroxyapatite).
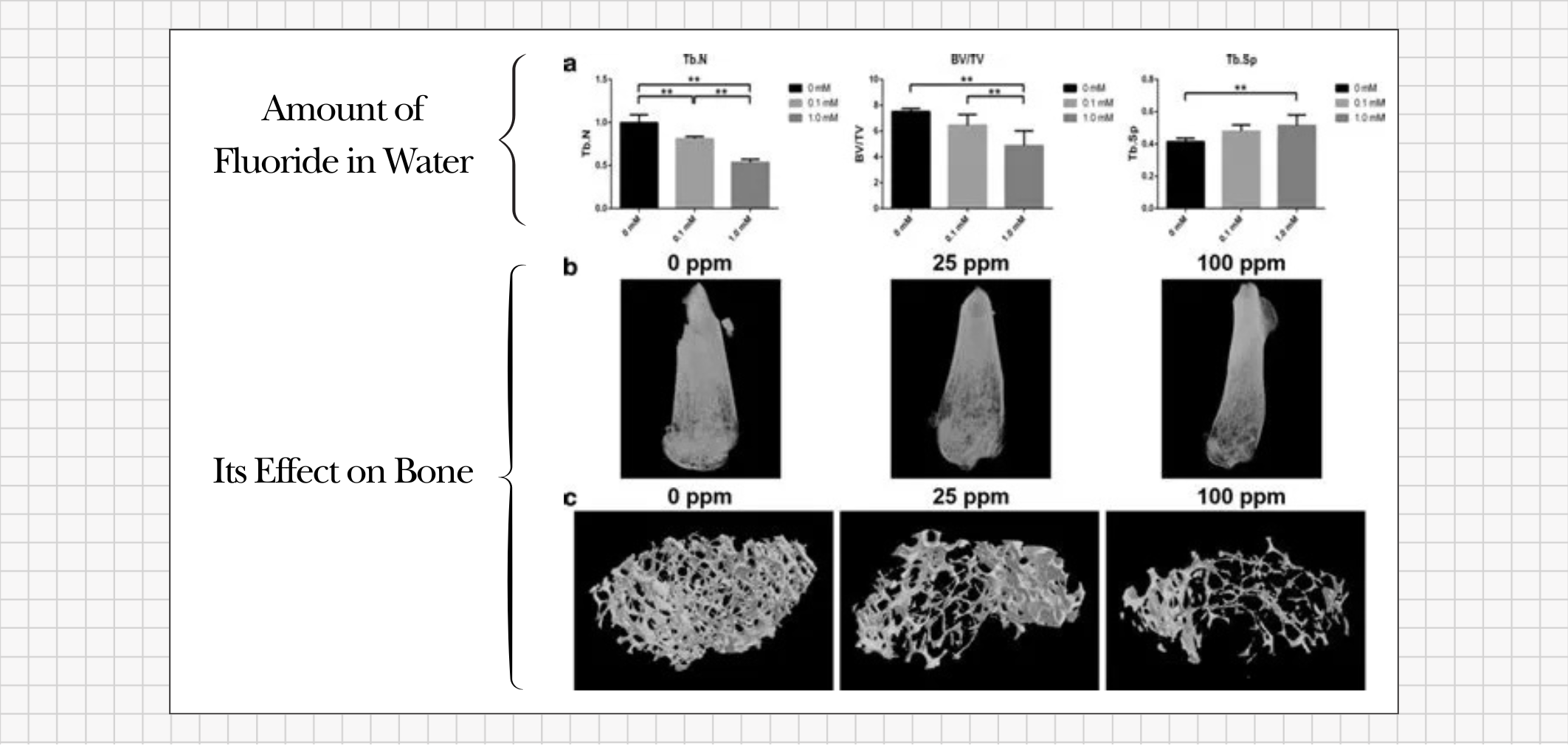
At first, a bone loaded with fluoride may appear denser on an X-ray because the extra mineral can increase bone mass. However, that density is misleading. Fluoride interferes with the bone-remodeling cycle and prompts new bone to form with abnormal structure. Instead of the smooth, healthy replacement of old bone, fluoride causes the bone to rebuild in a flawed way- producing bone that is more mineralized (hence denser) but riddled with structural defects.
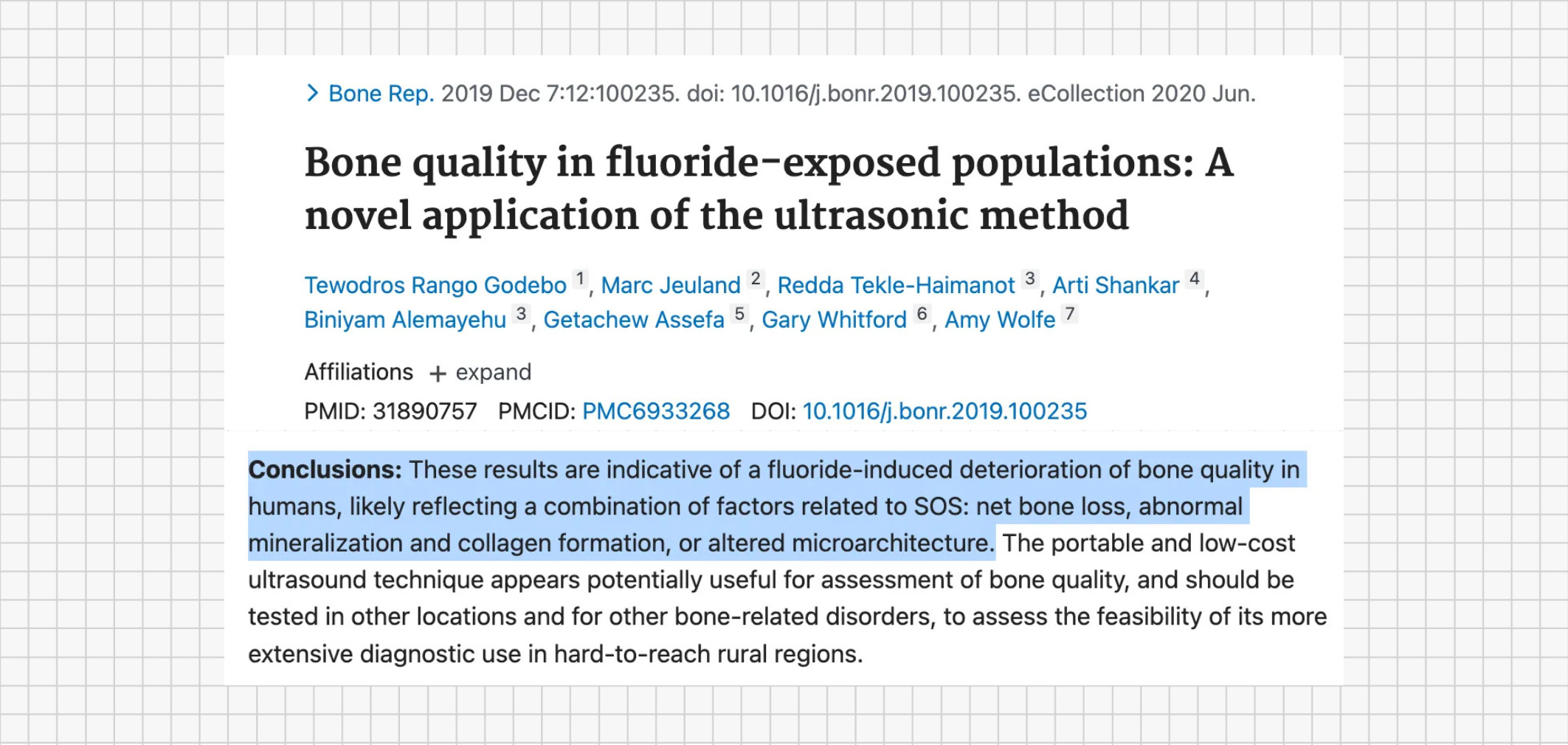
Imagine building a brick wall using brittle or misshapen bricks: the wall might look solid from the outside, but it will crack more easily under pressure. Similarly, under a microscope, bone affected by excess fluoride has larger, more imperfect mineral crystals and an imbalanced collagen-to-mineral ratio. In practical terms, this means the bone becomes harder but more brittle and prone to damage. Experts initially expected that adding fluoride into bone would strengthen it (since fluorapatite is a very hard mineral), but human studies have found this is not the case. Numerous studies have observed that while fluoride exposure can increase bone density, it does not translate into stronger bones. In fact, the new bone formed in the presence of excess fluoride is structurally weaker and more prone to fractures. In essence, fluoride in bone creates an illusion of strength (higher density on scans) while actually reducing the bone’s true resilience.

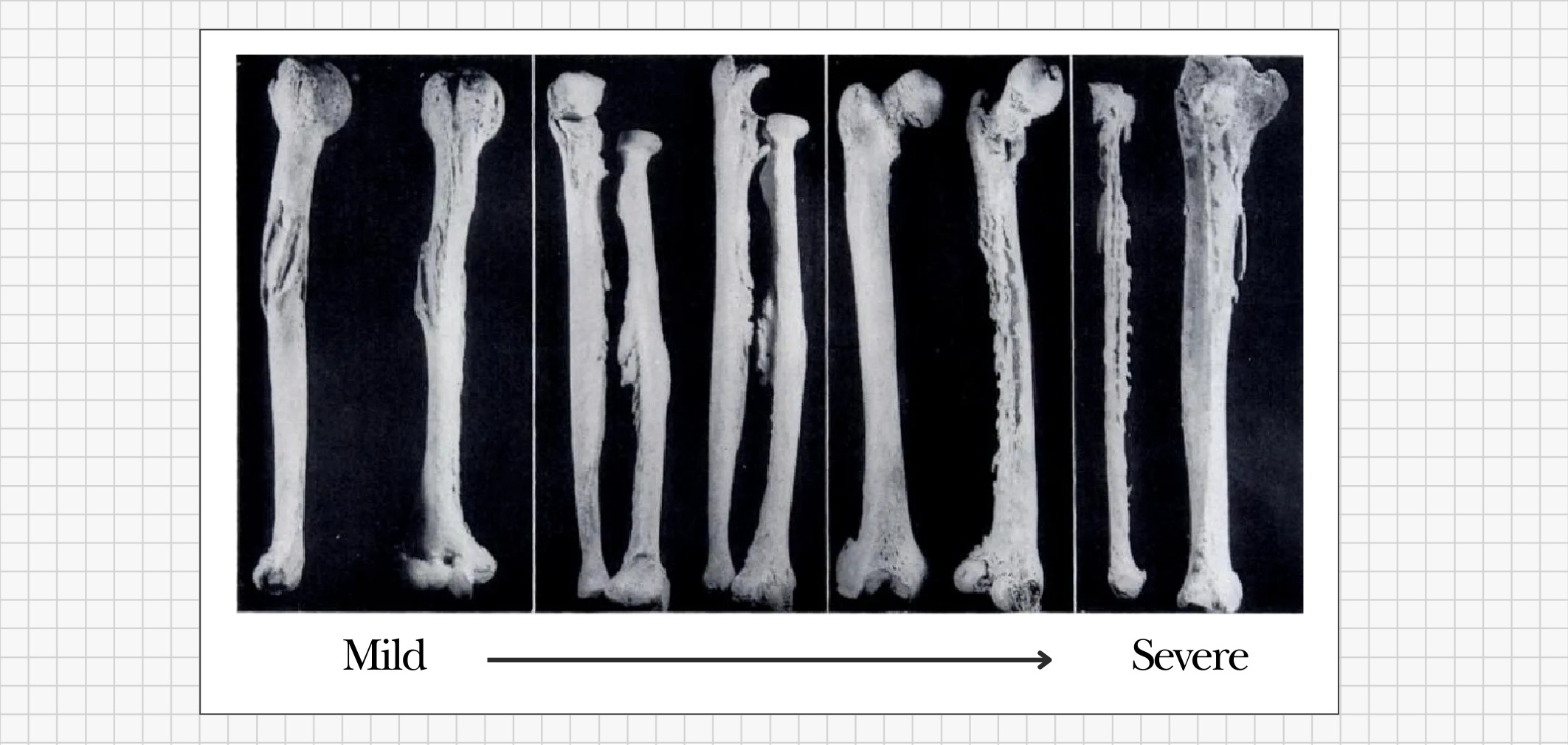
Fluoride’s harmful effects on bone don’t happen overnight - they build up gradually over decades. As more and more fluoride accumulates in the skeleton, skeletal fluorosis typically progresses through several stages of increasing severity:


Early Stage (Mild): Vague aches and stiffness begin to appear, often in the lower back, hips, knees, or neck. At this stage, someone might notice occasional joint pain or a stiff back, especially in the morning or after exercise. These subtle symptoms are easily mistaken for normal aging or everyday wear-and-tear. There are usually no obvious signs on X-rays yet, and bone density might even appear normal or only slightly increased.

Middle Stage (Moderate): With continued fluoride exposure, the symptoms become more pronounced and harder to ignore. Pain in the bones and joints grows more frequent, and movements that used to be easy – like bending, lifting, or climbing stairs – become increasingly difficult due to stiffness and pain. Ligaments and joint capsules may start to calcify (harden with mineral deposits), reducing flexibility. A person in this stage might have constant joint and back pain that doesn’t respond well to typical treatments. An X-ray at this point might show unusually dense bone patches or calcified ligaments around joints, although doctors might not immediately recognize these as signs of fluorosis.

Advanced Stage (Severe): After many years (often decades) of high fluoride accumulation, the damage can become crippling. Bones may thicken, deform, or develop odd bony outgrowths (exostoses). Joints can lose almost all mobility – for example, spinal vertebrae may enlarge and fuse together, and ligaments (especially in the spine and major joints) can ossify (literally turn to bone). The skeletal structure becomes so rigid that normal movement is profoundly limited. These changes can also compress nerves; for instance, hardened ligaments in the spine may pinch spinal nerves, leading to neurological symptoms like tingling, numbness, or weakness in the limbs. Muscles may waste away from disuse when movement becomes too painful or difficult. In extreme cases, a person may become nearly immobile – a condition historically known as crippling skeletal fluorosis. (In clinical reports, advanced fluorosis has led to patients becoming wheelchair-bound or bedridden due to multiple fractures and fused joints.)
▶︎ Key point: Skeletal fluorosis is a slow, progressive disease. What starts as mild stiffness and occasional aches can, over decades of fluoride accumulation, advance into severe joint deformities, constant pain, and loss of mobility.

One of the most troubling aspects of fluoride is that it is a cumulative toxin – the body does not excrete it efficiently. Each day, small exposures (from sources like fluoridated tap water, tea, or swallowed toothpaste) add a little more fluoride to your bones. Over time, these daily doses build up a significant reservoir of fluoride in the skeleton and joints.
Unlike many other toxins that the body can filter out in days or weeks, fluoride stays in bone for decades. Scientists estimate that once fluoride has built up in your bones, it has an extremely long biological half-life, on the order of 20 years or more. In other words, if you completely stopped ingesting any new fluoride today, roughly half of the fluoride stored in your bones would still be there 20 years from now.
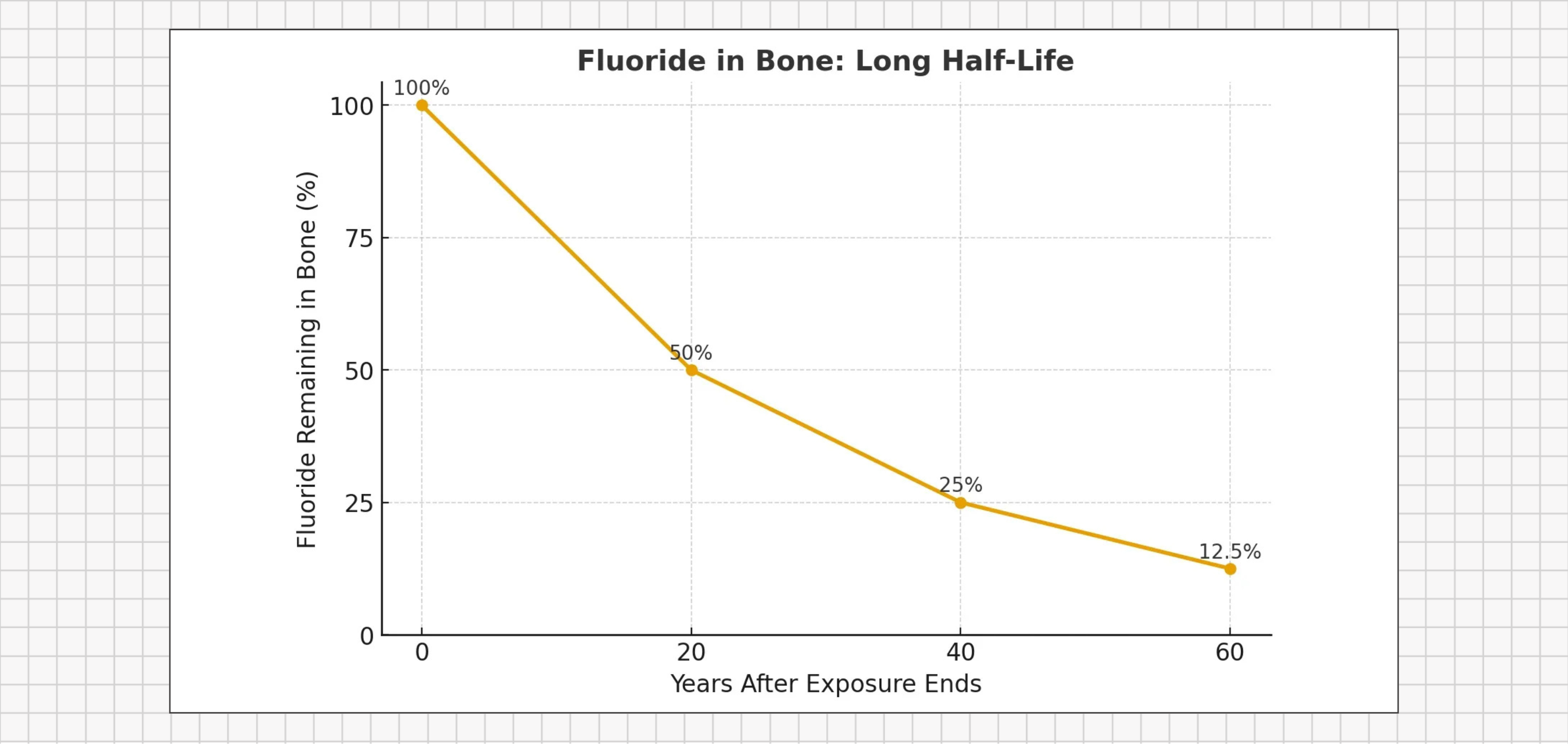
This glacial pace of fluoride clearance means that the fluoride accumulated in your 30s or 40s could still be affecting your bone health in your 60s and 70s. Real-world observations back this up. In one study, workers from a Swiss aluminum factory had very high fluoride exposure on the job. Years after these workers stopped being exposed (after retirement), researchers measured their bone fluoride levels. They found that even after two decades away from fluoride exposure, the workers’ bones had only lost about half of the fluoride they had accumulated. In essence, their skeletons were still carrying decades-old fluoride.
This extremely slow elimination explains why skeletal fluorosis sneaks up on people: it doesn’t appear suddenly, but rather builds silently year after year as fluoride progressively loads into the bones. By the time clear symptoms emerge, a vast amount of fluoride has been entrenched in the skeletal system for a long time.

The tragedy of skeletal fluorosis lies in its silence. Early symptoms creep in so gradually that most people (and even their doctors) mistake them for something else. Mild joint stiffness, occasional aches, or slightly brittle bones are almost always blamed on “just getting older” or common arthritis. Yet mounting research and clinical observations suggest that in some cases, these age-related complaints might actually be the early signs of fluoride’s accumulated burden on the body. The clinical symptoms of fluoride’s effect on bones are indistinguishable from arthritis in many cases. In fact, even relatively low-level fluoride exposure can contribute to or worsen these joint and bone problems, especially in people with certain nutritional predispositions. In other words, what looks like ordinary osteoarthritis or general aging could be something more preventable: fluoride slowly damaging the bones and joints.
Even at fluoride levels long considered “safe,” the buildup in our bones can be significant. The U.S. National Research Council has noted that at a water fluoridation level of about 1 part per million (ppm), a person’s skeleton could accumulate several thousand milligrams (i.e. multiple grams) of fluoride after just 10–20 years of exposure. Studies from India and China – countries with widespread fluorosis – have documented cases of skeletal fluorosis at water fluoride levels as low as 0.7–1.5 ppm. (For context, 0.7–1.0 ppm is the range of fluoride typically added to many U.S. and Canadian water supplies.) These findings challenge the long-held assumption in North America that skeletal fluorosis doesn’t occur at water fluoride levels below about 4 ppm. In light of the evidence, and considering that fluoride is not a nutrient our bodies require, it’s worth rethinking the notion that long-term fluoride exposure at commonly encountered levels is harmless.
Another harsh truth is that once fluoride is locked into your bones, the damage is essentially irreversible. There is no established medical treatment to remove fluoride from bone or to reverse the structural changes it causes. In advanced cases of fluorosis, even significantly reducing fluoride intake cannot undo calcified ligaments or fix long-standing bone deformities. Scientific reviews emphasize that once skeletal fluorosis has progressed, it cannot be “cured” in the usual sense – the focus must be on preventing excessive fluoride accumulation in the first place. Some improvement may occur if fluoride exposure is stopped early enough, because the body will slowly (over decades) excrete fluoride from bones, and bone remodeling can gradually replace some damaged bone with healthy bone. However, this is a very slow process and often only partial. In practical terms, that means the skeletal damage fluoride causes can last a lifetime.
In summary, what many people accept as “normal” aging – stiff joints, aches, and reduced mobility – may in some cases be a preventable condition. Just because a health problem develops slowly does not mean it’s harmless, and just because a condition has become common doesn’t mean it’s “normal.” Fluoride will leave its mark on the skeleton whether we notice it or not. By recognizing this silent accumulation for what it is, we have a chance to prevent future generations from carrying an invisible fluoride burden into their later years.

Completely avoiding fluoride in today’s world is challenging. It’s present in many water supplies, foods, and dental products - but you can take practical steps to lower your lifetime exposure and protect your bones. In fact, the same measures that prevent dental fluorosis in children can also help safeguard your bones from skeletal fluorosis:
Mind your water source: Whenever possible, drink and cook with water that is not fluoridated, or use a reliable water filtration system that removes fluoride. This is one of the most effective ways to reduce daily fluoride intake, since water and beverages made from water are major fluoride sources for many people. If you live in an area with fluoridated tap water, consider using filtered or non-fluoridated water for drinking and cooking, especially for young children or if you consume large volumes of water (e.g. athletes or outdoor workers).
Be careful with dental products: Choose fluoride-free toothpaste and mouth rinses, especially for young children. Many people (kids in particular) end up swallowing some toothpaste or mouthwash, inadvertently ingesting fluoride.
Watch for hidden fluoride in foods and drinks: Be aware that certain foods and beverages can contribute to your fluoride intake. Tea (made from tea leaves, which naturally accumulate fluoride), sodas and juices reconstituted with fluoridated water, and some processed foods or powders (soups, powdered drink mixes, reconstituted juice concentrates.) may contain significant fluoride. Some supplements and medications also contain fluoride. Read labels and opt for lower-fluoride alternatives when you can.
Support bone health through nutrition: Maintain a nutrient-rich diet that supports your bones. Adequate calcium and magnesium intake can help keep your mineral balance in check, potentially reducing how much fluoride your body retains (since calcium, for example, can compete with fluoride for absorption). Vitamins D and K2 are crucial for bone health and proper mineral utilization – they help ensure calcium goes into bones where it’s needed (and not into soft tissues). A strong nutritional foundation helps your body handle minerals properly and may mitigate some of fluoride’s impact.
Each of these choices may seem small, but they add up significantly over time. By reducing avoidable fluoride sources day by day, you can dramatically cut down the total amount of fluoride that accumulates in your bones in the long run. Starting early is especially important!
Coming Next: How fluoride disrupts thyroid health - interfering with iodine, slowing hormone production, and contributing to the growing epidemic of hypothyroidism.